
Have a mission, plan ahead, question everything, assume nothing, roll up your sleeves, study the past, take risks, dream higher, welcome change, have an amazing haircut, laugh, be curious, pay attention to details. make mistakes, think sideways, do things with passion, don’t forget to play, take it to the edge, breathe. Creativity takes courage.
Category: Post
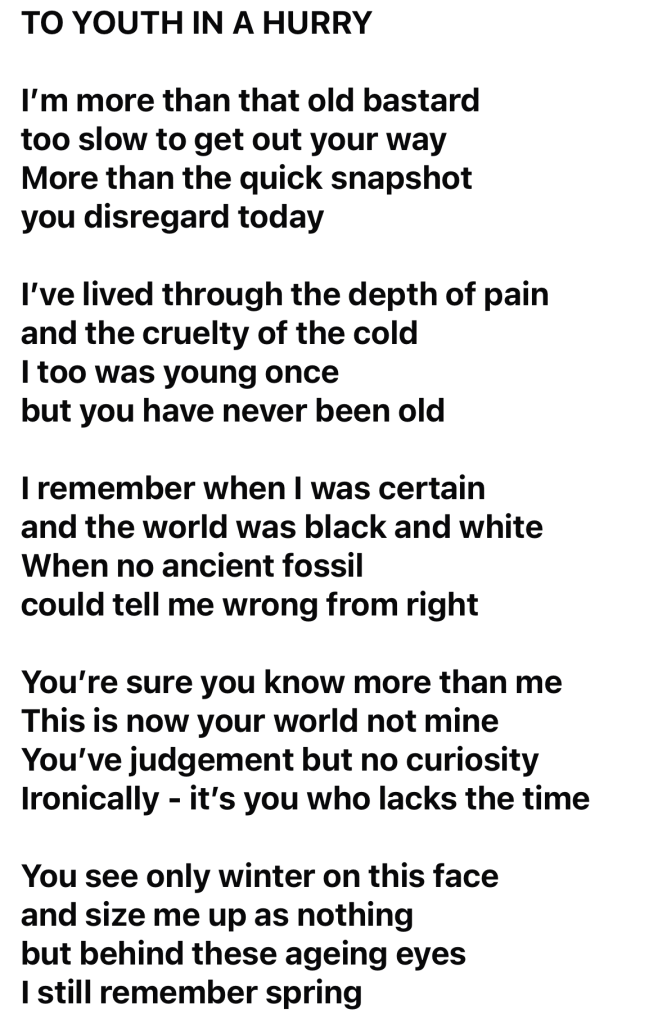
‘To Youth In A Hurry’ by Henry Normal
Stepping away from social media has brought a certain clarity and calm — but every so often, you miss something that makes you pause. This was one of those moments. An old friend wrote this, and it quietly stopped me in my tracks. I genuinely think this is beautiful…

The Contact Concept
Introducing Neighbourhood Contact Groups
Connecting communities in order to identify and mitigate rising risk of illness.
Across health and social care systems, we are seeing increasing complexity in need. Long-term conditions, frailty, musculoskeletal problems, mental health pressures, and social isolation are combining in ways that mean there is a rising risk of illness which often occurs unnoticed and only becomes visible once people present in crisis, usually to their local Emergency Department.
Integrated Neighbourhood Teams (INTs), particularly through the focus on early identification and mitigation of rising risk of illness, are being designed to respond to this challenge. However, identifying risk early is not something that is easily done and it could be argued that, historical health and social care arrangements have often been structurally ill-equipped to do so effectively.
Collaborative communities often recognise change before formal systems do. That insight underpins Neighbourhood Contact Groups — referred to here simply as “Contact” (on the basis that life is far too short for another three-letter acronym).
What is Contact?
Neighbourhood Contact Groups are locally based forums aligned to local neighbourhoods. Their purpose is straightforward:
To connect communities, enabling prompt identification and action on the rising risk of illness by collective mitigation, and stronger social resilience.
Contact is not another clinical meeting, nor is it a traditional multidisciplinary team (MDT) forum. It does not replace existing health and social care services. Instead, it creates a structured space in which residents, clinicians, care providers, voluntary sector partners, and local leaders come together to share insight, generate coordinated action, and strengthen prevention at neighbourhood level.
Contact’s premise is simple: prevention works best when it is connected, individualised, and relatable.
Why This Matters
Across both rural and urban settings, communities face shared pressures:
- Increasing prevalence of long-term conditions
- Growing multimorbidity
- Social isolation and loneliness
- Workforce pressures within primary and community services
- Escalating demand on urgent and acute care
Risk of illness frequently rises before it is formally recognised by local health services. By the time residents present to a healthcare professional, usually via an emergency department, opportunities for early mitigation may already have reduced.
Lived, relatable, and neighbourhood collaboration often provides the earliest signals of change. Yet this insight is rarely organised or integrated into health and social care systems in a meaningful way.
Contact seeks to provide that structure.
The Three Tenets of Contact
Neighbourhood Contact Groups are centred around three interconnected pillars:
1. Activity
Illness prevention begins with movement, interaction, and engagement.
Contact promotes accessible physical activity, structured wellbeing sessions, and purposeful community participation. Activity is not solely exercise, it is engagement, routine, connection, and agency, all of which are protective factors against rising health risk.
2. Health & Social Care
Contact creates collaboration between communities and neighbourhood health and social care teams.
Residents and local partners can share early concerns and emerging patterns, whether related to frailty, musculoskeletal issues, mental wellbeing, access challenges, or widening inequality. In return, clinicians and care professionals can offer early advice, signposting and providing routes into appropriate support.
Contact strengthens early intervention models by translating community intelligence into coordinated mitigation.
3. Community
Connection can improve health and, more importantly, prevent ill health.
By bringing people together regularly at a neighbourhood level, Contact reduces isolation, strengthens trust, and builds resilience. Stronger social and healthcare-related networks enable earlier informal support, improved self-management, and reduced reliance on crisis services.
Illness prevention is not solely a clinical concept, it is fundamentally social, driven by the environments in which people live and work.
How Contact Works
Neighbourhood Contact Groups operate as:
- Regular, community-led meetings
- Supported (but not dominated) by health and care professionals
- Structured around identifying emerging risk themes
- Focused on practical, local mitigations
- Connected into neighbourhood team escalation routes where needed
- Anchored by partnerships with voluntary and community organisations
The Contact model is deliberately designed to be simple, scalable, and flexible, enabling it to operate effectively across diverse settings, from rural communities to densely populated urban neighbourhoods.
What Success Would Look Like
If effective, Contact would contribute to:
- Earlier identification of rising risk of illness
- More proactive neighbourhood responses
- Increased participation in prevention and wellbeing activity
- Reduced avoidable escalation into urgent and acute care via ED
- Stronger community cohesion and resilience
In essence, Contact seeks to make illness prevention visible and participatory at neighbourhood level.
Contact | The Core Idea
Health risk does not emerge in isolation, and prevention should not either.
Neighbourhood Contact Groups bring together activity, health and social care, and community connection within a single, structured forum. By doing so, they offer a practical way to provide early health and social care intervention while reinforcing something equally important:
Contact.
Contact connects patients with communities of care, combining shared intelligence, activity and human connection to provide and mitigate prompt action on rising risk of illness.

References:
Everett, J.A.C. (2013) ‘Intergroup Contact Theory: Past, Present, and Future’, In‑Mind Magazine, Issue 17.
Rathore, N. (2025) ‘The Fascinating Roots of the Contact Hypothesis’, Psywellpath Glossary.
Zuma, B. (2014) ‘Contact Theory and the Concept of Prejudice: Metaphysical and Moral Explorations’, Academia.edu.
Clinical Innovation Hub 2026
I’m looking forward to speaking at the Clinical Innovation Hub on the 3rd March 2026 where we will be discussing innovative solutions to improve our organisations’ operational efficiencies. Excited to network, discuss and strategise with my colleagues and peers in attendance. To view further information on the forum and how to attend please visit: Clinical Innovation Hub

2025 Global Forum

It was a great pleasure to attend and present at the 2025 Global Forum today. Thank you to Sprink and The Scottish Government for inviting me.

Healthcare Strategy Forum 2025


Healthcare Strategy Forum 2025
I’m looking forward to speaking at the Healthcare Strategy Forum on the 18th & 19th November where we will be discussing innovative solutions to improve our organisations’ operational efficiencies. Excited to network, discuss and strategise with my colleagues and peers in attendance. To view further information on the forum and how to attend please visit: https://www.healthcarestrategyforum.com/

EQ-5D or MSK-HQ: A commissioning decision
The EQ-5D and the MSK-HQ are both tools used to measure health outcomes, but they serve different purposes and have distinct characteristics. From a commissioner’s perspective in the UK, understanding the key differences between these two instruments is crucial for making informed decisions about healthcare provision and evaluation.
The EQ-5D is a standardised instrument used to measure general health-related quality of life. It is designed to be applicable to a wide range of health conditions and treatments. The EQ-5D includes five dimensions: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. It also includes a visual analogue scale (VAS) for the patient to rate their overall health.
Advantages of the EQ-5D include its versatility, being applicable to a wide range of diseases and health states, not limited to any specific condition. It allows for comparison across different diseases and treatments, generates utility values that can be used in health economic evaluations including cost-utility analysis, and is widely accepted and used in clinical trials, health surveys, and economic evaluations globally. However, its generic nature might not capture condition-specific details and nuances, and it may be less sensitive to changes in specific conditions such as musculoskeletal disorders compared to condition-specific instruments.
On the other hand, the MSK-HQ is a condition-specific questionnaire designed to measure health outcomes in patients with musculoskeletal (MSK) conditions. It focuses specifically on MSK conditions, including back pain, arthritis, and other musculoskeletal disorders. The MSK-HQ includes 14 items covering pain, physical function, physical activity, sleep, fatigue, emotional well-being, and social participation.
The MSK-HQ’s advantages include its condition-specific focus, which captures the specific issues and outcomes relevant to patients with musculoskeletal conditions. It is more sensitive to changes in health status related to MSK conditions, allowing for more detailed tracking of patient progress and outcomes. Developed with input from patients and clinicians, it ensures coverage of the aspects most important to those with MSK conditions. However, its limited scope makes it unsuitable for use with non-MSK conditions, limiting its applicability in a broader healthcare context. It is less useful for comparing across different types of diseases and treatments outside of MSK conditions, and it does not generate utility values for economic evaluations, limiting its use in cost-utility analyses.
From a commissioner’s perspective, the key differences between the EQ-5D and the MSK-HQ are clear. In terms of applicability, the EQ-5D is suitable for a broad range of health conditions, making it useful for general health assessments and comparisons across different patient groups. The MSK-HQ, however, is specifically designed for musculoskeletal conditions, providing more detailed and relevant information for this patient population. In terms of sensitivity and specificity, the EQ-5D may lack sensitivity for specific conditions, potentially missing important changes in health status in patients with MSK conditions, whereas the MSK-HQ is more sensitive to changes in musculoskeletal health, providing more precise information on patient outcomes in this area.
For economic evaluations, the EQ-5D generates utility values that are essential for cost-utility analysis and economic evaluations in healthcare. In contrast, the MSK-HQ does not provide utility values, limiting its use in economic evaluations. In terms of use cases, the EQ-5D is ideal for broad applications, including public health surveys, clinical trials, and general health assessments. The MSK-HQ is best suited for clinical settings focused on musculoskeletal conditions, rehabilitation programs, and MSK-specific patient monitoring.
Considering patient-centred outcomes, the EQ-5D is more general and may not capture all patient-specific concerns related to musculoskeletal conditions. The MSK-HQ, being developed with direct input from patients and clinicians dealing with MSK conditions, addresses the most relevant aspects of health and quality of life for these patients.
From a commissioner’s perspective, the choice between the EQ-5D and the MSK-HQ depends on the specific needs of the health service being provided. If the goal is to measure health outcomes across a broad range of conditions and perform economic evaluations, the EQ-5D is more appropriate. However, if the focus is on musculoskeletal health, the MSK-HQ provides more detailed and sensitive information that can better inform clinical decisions and patient care strategies.
The EQ-5D and the MSK-HQ are both tools used to measure health outcomes, but they serve different purposes and have distinct characteristics. From a commissioner’s perspective in the UK, understanding the key differences between these two instruments is crucial for making informed decisions about healthcare provision and evaluation.
The EQ-5D is a standardised instrument used to measure general health-related quality of life. It is designed to be applicable to a wide range of health conditions and treatments. The EQ-5D includes five dimensions: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. It also includes a visual analogue scale (VAS) for the patient to rate their overall health.
Advantages of the EQ-5D include its versatility, being applicable to a wide range of diseases and health states, not limited to any specific condition. It allows for comparison across different diseases and treatments, generates utility values that can be used in health economic evaluations including cost-utility analysis, and is widely accepted and used in clinical trials, health surveys, and economic evaluations globally. However, its generic nature might not capture condition-specific details and nuances, and it may be less sensitive to changes in specific conditions such as musculoskeletal disorders compared to condition-specific instruments.
On the other hand, the MSK-HQ is a condition-specific questionnaire designed to measure health outcomes in patients with musculoskeletal (MSK) conditions. It focuses specifically on MSK conditions, including back pain, arthritis, and other musculoskeletal disorders. The MSK-HQ includes 14 items covering pain, physical function, physical activity, sleep, fatigue, emotional well-being, and social participation.
The MSK-HQ’s advantages include its condition-specific focus, which captures the specific issues and outcomes relevant to patients with musculoskeletal conditions. It is more sensitive to changes in health status related to MSK conditions, allowing for more detailed tracking of patient progress and outcomes. Developed with input from patients and clinicians, it ensures coverage of the aspects most important to those with MSK conditions. However, its limited scope makes it unsuitable for use with non-MSK conditions, limiting its applicability in a broader healthcare context. It is less useful for comparing across different types of diseases and treatments outside of MSK conditions, and it does not generate utility values for economic evaluations, limiting its use in cost-utility analyses.
From a commissioner’s perspective, the key differences between the EQ-5D and the MSK-HQ are clear. In terms of applicability, the EQ-5D is suitable for a broad range of health conditions, making it useful for general health assessments and comparisons across different patient groups. The MSK-HQ, however, is specifically designed for musculoskeletal conditions, providing more detailed and relevant information for this patient population. In terms of sensitivity and specificity, the EQ-5D may lack sensitivity for specific conditions, potentially missing important changes in health status in patients with MSK conditions, whereas the MSK-HQ is more sensitive to changes in musculoskeletal health, providing more precise information on patient outcomes in this area.
For economic evaluations, the EQ-5D generates utility values that are essential for cost-utility analysis and economic evaluations in healthcare. In contrast, the MSK-HQ does not provide utility values, limiting its use in economic evaluations. In terms of use cases, the EQ-5D is ideal for broad applications, including public health surveys, clinical trials, and general health assessments. The MSK-HQ is best suited for clinical settings focused on musculoskeletal conditions, rehabilitation programs, and MSK-specific patient monitoring.
Considering patient-centred outcomes, the EQ-5D is more general and may not capture all patient-specific concerns related to musculoskeletal conditions. The MSK-HQ, being developed with direct input from patients and clinicians dealing with MSK conditions, addresses the most relevant aspects of health and quality of life for these patients.
From a commissioner’s perspective, the choice between the EQ-5D and the MSK-HQ depends on the specific needs of the health service being provided. If the goal is to measure health outcomes across a broad range of conditions and perform economic evaluations, the EQ-5D is more appropriate. However, if the focus is on musculoskeletal health, the MSK-HQ provides more detailed and sensitive information that can better inform clinical decisions and patient care strategies.
The Benefits of Community-Based Musculoskeletal Interface Services in the NHS: A Patient’s Perspective
Living with a musculoskeletal (MSK) condition can significantly impact a patient’s quality of life. MSK conditions, which affect muscles, bones, and joints, are common and can range from acute injuries to chronic syndromes like fibromyalgia. For NHS patients, the integration of community-based MSK interface services has been transformative.
1. Accessibility and Convenience
Community-based MSK services are designed to be closer to home, reducing travel time and providing easier access to care. This is especially beneficial for patients with mobility issues or chronic pain, as it alleviates the stress and fatigue associated with long journeys to hospitals. Additionally, local clinics often offer more flexible appointment times, better accommodating work and personal schedules.
2. Timely Care and Reduced Waiting Times
A significant benefit of community-based services is the reduction in waiting times. Traditional hospital-based MSK services often have long waiting lists, causing delays in diagnosis and treatment. In contrast, community-based services streamline the process with quicker initial assessments and faster referrals to specialists if needed. This timely intervention can prevent conditions from worsening, leading to better outcomes and a quicker return to normal activities.
3. Personalised and Holistic Care
Community-based MSK services tend to adopt a holistic approach to patient care. Practitioners in these settings often have the time to engage more deeply with patients, understanding their personal circumstances and tailoring treatments accordingly. This patient-centered approach ensures that care plans are not only medically appropriate but also practical and achievable for the individual’s lifestyle.
4. Integrated Multi-Disciplinary Teams
Community MSK services are typically staffed by a multi-disciplinary team of healthcare professionals, including physiotherapists, occupational therapists, GPs with a special interest in MSK conditions, and sometimes mental health specialists. This integrated team approach ensures that patients receive comprehensive care that addresses all aspects of their condition. For instance, physiotherapists can provide exercises to improve mobility, while occupational therapists can suggest modifications to everyday activities to reduce pain and strain.
5. Enhanced Patient Education and Self-Management
Empowering patients with knowledge about their conditions and involving them in their treatment plans is a cornerstone of community-based care. These services often provide educational resources and self-management support, teaching patients exercises and strategies to manage symptoms independently. This not only improves patient outcomes but also reduces dependency on healthcare services, fostering a sense of control and confidence in managing one’s health.
6. Stronger Community Connections
Receiving care within the community fosters a sense of belonging and support. Patients often benefit from peer support groups and local resources that offer additional help and encouragement. Knowing that others in the community are going through similar experiences can be incredibly reassuring and motivating, aiding in mental and emotional wellbeing.
7. Cost-Effectiveness
From a broader perspective, community-based MSK services are cost-effective for the NHS. By reducing the burden on hospital services and preventing the progression of conditions through early intervention, these services help manage healthcare resources more efficiently. This, in turn, ensures the sustainability of the NHS and the continued provision of high-quality care for all.
Conclusion
For patients, the shift to community-based MSK interface services has been overwhelmingly positive. The combination of accessibility, timely care, personalised treatment, integrated support, patient education, and community connection creates a robust framework for effectively managing musculoskeletal conditions. These benefits underscore the importance of continued investment and expansion of community-based MSK services within the NHS, ultimately enhancing patient experiences and outcomes.
The Narrative of Analysis

